
Bedsores: Types and Nursing Management
Introduction
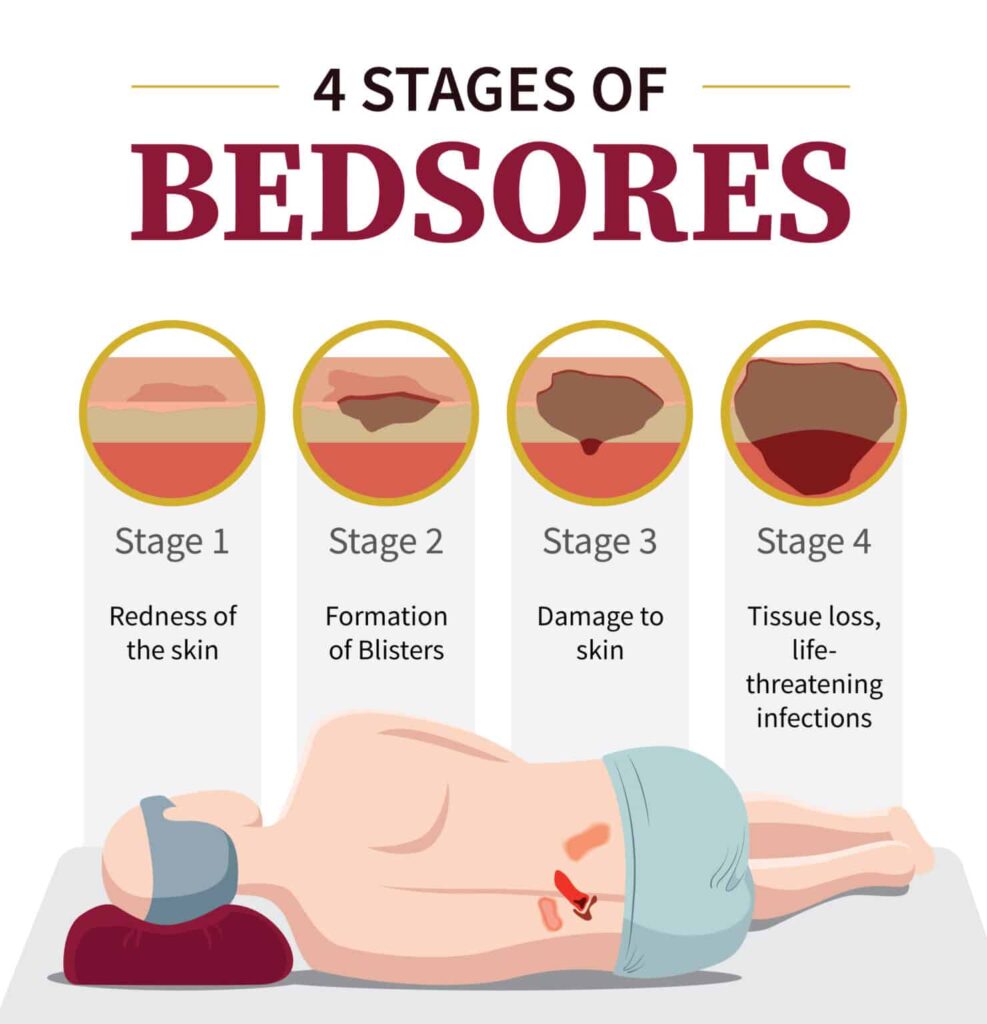
Bedsores, also known as pressure ulcers, pressure injuries, or decubitus ulcers, are localized injuries to the skin and underlying tissues that occur due to prolonged pressure, friction, or shear. They commonly develop in patients who are immobile, bedridden, wheelchair-bound, or critically ill. Bedsores are a major concern in hospitals, long-term care facilities, and home care settings, as they increase patient morbidity, prolong hospital stay, raise healthcare costs, and significantly reduce quality of life. There are 4 stages of bedsores
Nurses play a vital role in the prevention, early identification, and management of bedsores. Proper nursing care can prevent most pressure ulcers and promote healing when they occur. This blog discusses the types of bedsores and outlines comprehensive nursing management strategies.
What Are Bedsores?
Bedsores occur when continuous pressure on the skin reduces blood flow to the tissues. Without adequate blood supply, tissues become ischemic, leading to cell death and tissue breakdown. Bedsores usually develop over bony prominences such as the sacrum, heels, hips, elbows, ankles, shoulders, and back of the head.
Causes and Risk Factors
Causes
Prolonged pressure
Friction from bed linens or clothing
Shear forces during repositioning
Moisture from sweat, urine, or feces
Risk Factors
Immobility or paralysis
Advanced age
Poor nutrition and dehydration
Reduced sensory perception
Incontinence
Chronic illnesses (diabetes, vascular disease)
Poor circulation
Low body weight or obesity
Common Sites of Bedsores
Sacrum and coccyx
Heels and ankles
Hips
Elbows
Shoulder blades
Back of the head
Knees (in side-lying position)
4 Stages of Bedsores
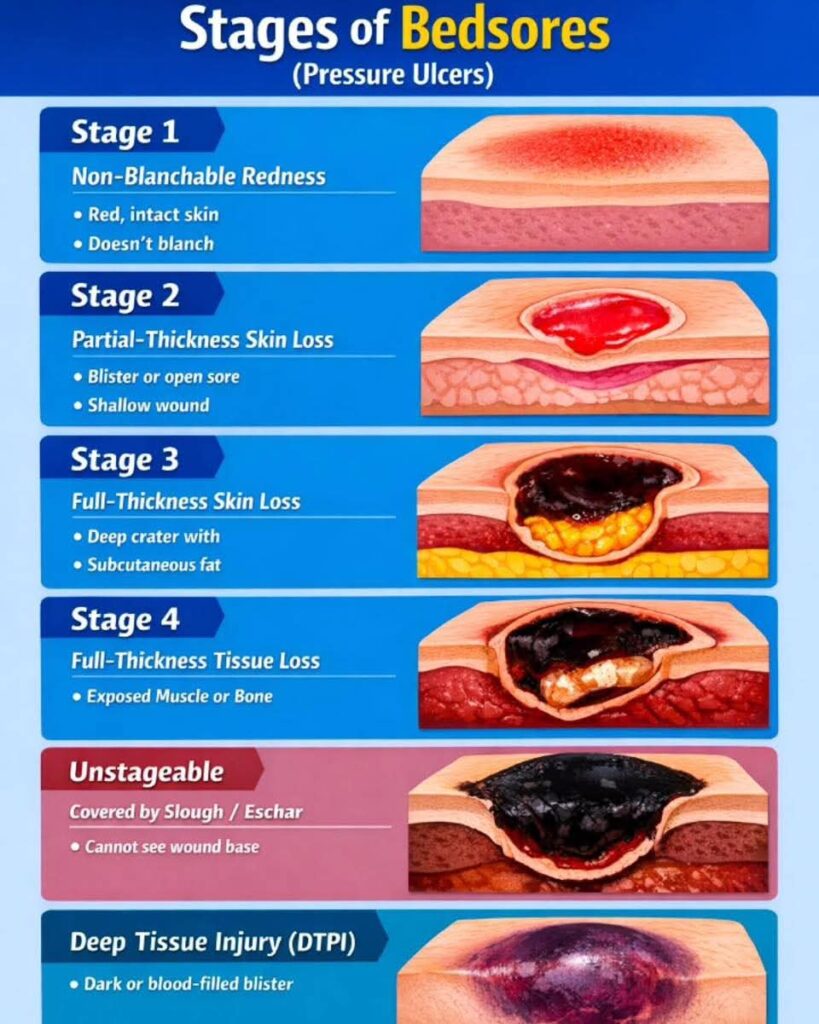
Stage 1: Non-Blanchable Erythema
Description:
Skin is intact
Persistent redness that does not blanch when pressed
Area may feel warm, firm, soft, or painful
Nursing Implications:
Early warning sign
Completely reversible if managed promptly
Stage 2: Partial-Thickness Skin Loss
Description:
Loss of epidermis and part of dermis
Appears as a shallow open ulcer
May present as a blister (intact or ruptured)
Red or pink wound bed
Nursing Implications:
Requires protective dressings
High risk of infection if not managed properly
Stage 3: Full-Thickness Skin Loss
Description:
Damage extends through the dermis into subcutaneous tissue
Fat may be visible
Slough may be present
No exposure of bone, tendon, or muscle
Nursing Implications:
Requires advanced wound care
Healing is slow
High risk of complications
Stage 4: Full-Thickness Tissue Loss
Description:
Extensive tissue destruction
Exposed bone, tendon, or muscle
Often includes slough or eschar
High risk of osteomyelitis and sepsis
Nursing Implications:
Medical and surgical intervention required
Long-term care and monitoring essential
Unstageable Pressure Injury
Description:
Wound base covered by slough or eschar
True depth cannot be determined
Deep Tissue Pressure Injury
Description:
Persistent dark red, maroon, or purple discoloration
Skin may be intact or non-intact
Indicates deep tissue damage
Nursing Management of Bedsores
1. Prevention of Bedsores
a. Risk Assessment
Use standardized tools such as the Braden Scale
Assess on admission and regularly thereafter
Identify high-risk patients early
b. Repositioning
Reposition bedridden patients every 2 hours
Reposition wheelchair-bound patients every 15–30 minutes
Use proper lifting techniques to reduce shear and friction
c. Pressure-Relieving Devices
Use air mattresses, foam mattresses, gel cushions
Place pillows under pressure points
Elevate heels using heel protectors
d. Skin Care
Inspect skin daily, especially bony prominences
Keep skin clean and dry
Use mild soap and moisturizers
Avoid vigorous massage over bony areas
e. Nutrition and Hydration
Ensure adequate protein intake
Encourage fluids unless contraindicated
Collaborate with dietitians
Monitor weight and nutritional status
f. Incontinence Management
Use absorbent pads
Provide timely toileting
Apply moisture barrier creams
2. Assessment of Bedsores
Measure wound size, depth, and location
Assess wound bed (color, slough, necrosis)
Check for signs of infection (redness, odor, discharge)
Monitor pain level
Document findings accurately and consistently
3. Treatment and Wound Care
a. Cleaning the Wound
Clean with normal saline
Avoid harsh antiseptics unless prescribed
Maintain aseptic technique
b. Dressing Selection
Stage 1: Protective films or hydrocolloids
Stage 2: Foam or hydrocolloid dressings
Stage 3 & 4: Alginate, foam, or antimicrobial dressings
Change dressings as per wound condition
c. Debridement
Removal of dead tissue
Types: Autolytic, enzymatic, mechanical, or surgical
Performed under medical supervision
d. Infection Control
Observe for systemic and local signs of infection
Administer antibiotics as prescribed
Maintain strict hand hygiene
4. Pain Management
Assess pain regularly using pain scales
Administer analgesics as prescribed
Provide comfort measures
Handle wounds gently during dressing changes
5. Mobility and Rehabilitation
Encourage active or passive range-of-motion exercises
Collaborate with physiotherapists
Promote early mobilization when possible
6. Patient and Family Education
Teach importance of frequent repositioning
Educate on skin inspection
Explain nutrition’s role in healing
Instruct caregivers on proper lifting and hygiene
Encourage reporting of early signs of pressure injury
Complications of Bedsores
Infection
Cellulitis
Osteomyelitis
Sepsis
Delayed wound healing
Increased mortality
Role of Nurses in Bedsores Management
Nurses are central to pressure ulcer care. Their responsibilities include:
Early risk identification
Implementation of preventive strategies
Ongoing wound assessment
Coordinating multidisciplinary care
Educating patients and caregivers
Advocating for patient comfort and dignity
Conclusion
Bedsores are largely preventable, yet they remain a significant healthcare challenge. Early detection, meticulous nursing care, proper nutrition, and consistent repositioning are the pillars of effective pressure ulcer management. Nurses play a crucial role in reducing the incidence and severity of bedsores through vigilant assessment, evidence-based interventions, and compassionate care. With proper nursing management, patients can experience faster healing, fewer complications, and an improved quality of life.